
Midodrine Use in Hemodialysis: An Opinion Editorial
Midodrine is often prescribed to patients on maintenance hemodialysis to manage low blood pressure during dialysis sessions. The clinical study we’re looking at raises many interesting points about the use of midodrine as a therapeutic option. In this editorial, we take a closer look at the evidence, explore the tricky parts of hemodialysis hypotension management, and offer a perspective on how clinicians might best steer through this challenging area.
The study in question tested the association between midodrine and patient outcomes such as overall mortality and cardiovascular events. Although the data were collected from a large real-world cohort, many of the findings remind us of the tangled issues that we face when treating patients whose clinical conditions are full of problems. Today, we will dig into the fine points of midodrine prescription and discuss why a measured, patient-centered approach is essential.
Understanding Midodrine’s Role in Blood Pressure Management During Hemodialysis
For many patients undergoing hemodialysis, intradialytic hypotension (IDH) is a nerve-racking complication characterized by a drop in blood pressure during treatment. Because of impaired compensatory mechanisms such as sympathetic tone and plasma refilling, patients are at risk of experiencing the dangerous twists and turns of low blood pressure. Midodrine, a prodrug that becomes desglymidodrine in the body, works by stimulating alpha-1 adrenergic receptors and thereby constricting blood vessels. This vasoconstrictive effect helps to increase blood pressure, making midodrine one of the key drugs in the clinical toolbox for this issue.
Yet, it is important to note that while midodrine may be effective in raising blood pressure, the clinical outcomes associated with its long-term use are not entirely clear. Although midodrine can provide quick relief, its impact on overall survival and cardiovascular events has been observed to vary according to different dose levels and patient conditions. The debate continues as to whether midodrine simply treats the symptom or if its use is a marker for more serious underlying issues.
Examining the Dose-Dependent Effects of Midodrine
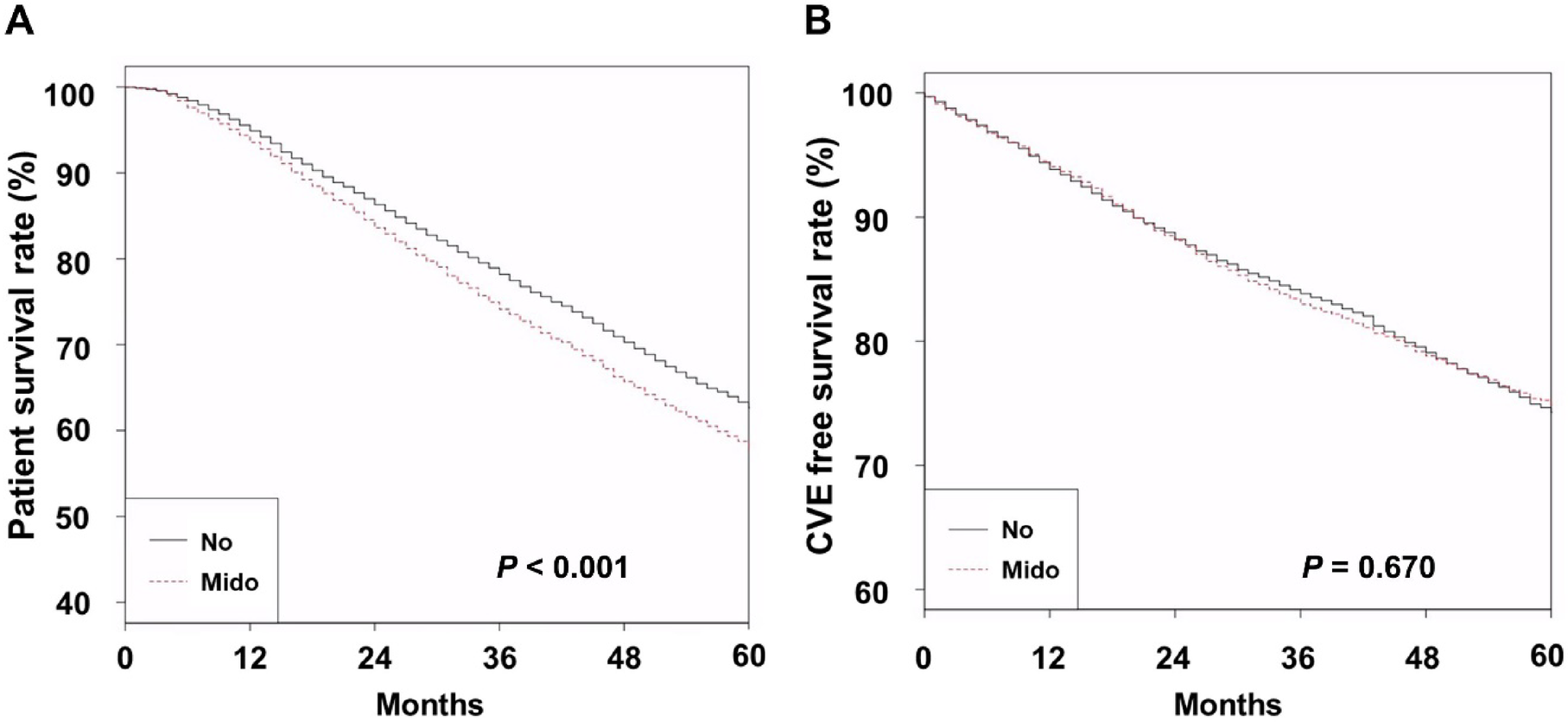
A particularly interesting aspect of the study is its finding that the higher the dose of midodrine, the greater the risk of all-cause mortality among hemodialysis patients. In the study, patients were divided into groups based on their midodrine prescriptions. For instance, those who received a high dose (defined as 30 or more pills over a six-month period) had worse survival outcomes compared to patients with no prescription or those who received a lower dose.
This dose-dependent relationship brings several tricky parts to the surface. One possibility is that patients requiring a higher dose of midodrine might already be at a higher risk because of more frequent or severe episodes of intradialytic hypotension. In this light, midodrine use becomes a marker for the extent of the problem rather than a direct cause of poorer outcomes.
However, the study controlled for many patient characteristics and comorbidities with detailed propensity score matching. Even after adjusting for these complicated pieces of variation, midodrine remained associated with a considerable increase in mortality risk. Here is a simplified table summarizing the key points:
| Group | 5-Year Survival Rate | Risk of Mortality (HR) |
|---|---|---|
| No midodrine prescription | 62.6% | Reference |
| Low-dose midodrine | Approximately similar to the reference value | Slight difference (not statistically significant) |
| High-dose midodrine | 55.3% | Significantly higher, adjusted HR around 1.16 |
From this data, it is clear that careful attention must be paid to the dose of midodrine prescribed. This observation also suggests that oversimplifying the treatment by solely focusing on blood pressure may not be the best approach. Instead, clinicians must consider the entire clinical picture—including the frequency of intradialytic hypotensive episodes, the presence of other cardiovascular conditions, and overall patient frailty.
The Tricky Parts of Hemodialysis Hypotension Management
Managing intradialytic hypotension is not just about administering a drug; it involves working through a series of interconnected issues that are as complex as they are intimidating. Some of the confusing bits include:
- Underlying Cardiovascular Autonomic Dysfunction: Many patients on hemodialysis have impaired autonomic function. This can make their response to volume shifts during dialysis unpredictable.
- Fluid Management and Ultrafiltration Volume: Achieving the right balance between fluid removal and hemodynamic stability is a constant struggle. Too aggressive fluid removal can lead to IDH, and too little removal can exacerbate other complications.
- Blood Pressure Variability: The changes in blood pressure during dialysis are not only affected by midodrine but also by other medications like anti-hypertensive drugs. This variability may be linked to increased mortality in some cases.
- Comorbidities and Overall Health: Patients with diabetes, heart failure, or other cardiovascular conditions may have hidden complexities that influence the response to midodrine therapy.
Each of these points represents a small twist in the broader picture of managing hypotension in this vulnerable population. When the delicate balance of blood pressure is upset, clinicians must not only treat the symptom but also dive into the underlying causes.
Patient Outcomes and the Clinical Dilemma
One cannot ignore the fact that midodrine use appears to correlate with worse overall survival. This association has led many to wonder whether prescribing midodrine is inadvertently leading to a worse clinical outcome or if its use is merely a signal of advanced underlying disease. It is likely that both factors play a role.
Critics of aggressive midodrine use argue that while it may offer temporary relief, it might also contribute to increased peripheral vascular resistance, potentially impairing tissue perfusion. For instance, if the vasoconstriction from midodrine is too pronounced, it might result in a decrease in cardiac output. This could particularly affect patients whose cardiac function is already compromised by underlying conditions.
On the other hand, it is important to remember that the choice to prescribe midodrine is rarely made in isolation. Clinicians take into account multiple facets of the patient’s health status. In many cases, the use of midodrine might simply highlight a patient who is generally sicker and therefore at higher risk of complications. This phenomenon, sometimes referred to as “confounding by severity,” complicates efforts to ascertain a direct cause-and-effect relationship.
Overall, these findings advise caution. They suggest that while midodrine might be helpful for managing the immediate drop in blood pressure, its long-term use should prompt clinicians to explore additional strategies to address the overall condition of the patient.
Integrating Alternative Approaches for Managing Hypotension
Given the potential issues associated with midodrine, it is essential that healthcare professionals consider an integrative approach to managing intradialytic hypotension. This means blending pharmacological intervention with non-pharmacological strategies. Many clinicians are beginning to rely on a more holistic approach that includes the following:
- Dialysate Cooling: Cooling the dialysate can help maintain blood pressure stability during dialysis sessions by moderating the temperature-induced vasodilation.
- Adjusting Ultrafiltration Rates: Tailoring the fluid removal rate to avoid too rapid shifts in blood volume reduces the risk of IDH while also ensuring effective fluid management.
- Optimizing Dialysis Session Duration: Extending the duration of dialysis can allow for a gentler fluid removal process, potentially reducing the incidence of hypotensive events.
- Lifestyle and Dietary Adjustments: Educating patients about ways to manage interdialytic weight gain through dietary measures can be critical. This may include moderating salt intake, monitoring fluid consumption, and scheduling meals thoughtfully around dialysis sessions.
The following table summarizes various strategies and their intended benefits:
| Strategy | Benefit |
|---|---|
| Dialysate Cooling | Helps maintain vascular tone and reduces blood pressure drops |
| Fluid Removal Adjustments | Minimizes rapid shifts in blood volume and lessens hypotensive episodes |
| Extended Dialysis Sessions | Allows for gentler change in fluid status and better hemodynamic stability |
| Dietary Modifications | Reduces interdialytic weight gain and associated blood pressure variability |
It is clear that midodrine represents only one component of a much broader strategy. Health professionals must consider these alternative approaches while also ensuring that the patient’s overall medical condition is optimally managed.
Fine-Tuning Treatment Protocols Amid Confusing Clinical Bits
One of the greatest challenges in the field of dialysis is figuring a path through the tangled issues associated with treatment protocols. The current evidence suggests that midodrine should be prescribed with caution; its use, especially at high doses, is linked to increased mortality. However, this doesn’t necessarily mean that the drug has no place in therapy.
Instead, the subtle parts of patient management lie in integrating midodrine with other measures designed to optimize cardiovascular health. A few practical suggestions include:
- Frequent Monitoring: Keep an eye on blood pressure variability during dialysis sessions, and adjust treatment parameters as needed.
- Individualized Dosing: Treat each patient as unique; what works safely for one may pose risks for another especially if there are several comorbid conditions present.
- Combination Therapy: Consider combining midodrine with non-pharmacological strategies (like dialysate cooling) to reduce the overall reliance on drugs.
- Regular Assessment of Cardiovascular Health: Since many patients undergoing hemodialysis have an underlying burden of cardiovascular disease, routine evaluation can help in early identification of issues that may worsen with midodrine use.
In short, healthcare providers should actively search for and promptly treat comorbidities and risk factors that complicate blood pressure management. Stepping beyond the simple goal of elevating blood pressure, clinicians must strive to ensure overall improvements in survival and quality of life.
Impact on Cardiovascular Events: What Do We Really Know?
While the study found a clear relationship between midodrine use and overall mortality, the connection with cardiovascular events (CVEs) is less straightforward. In the analysis, the CVE-free survival rates did not differ significantly among patients with varied midodrine dosing, suggesting that the drug’s impact might be specific to non-atherosclerotic mechanisms.
One plausible explanation is that midodrine may contribute more to complications such as reduced tissue perfusion or cardiac arrhythmias rather than directly increasing the risk of heart attacks or strokes.
Subgroup analyses by comorbidity burden revealed an interesting pattern: in patients with fewer health complications, midodrine might even be associated with a reduced CVE risk, whereas patients with a heavy comorbidity load experienced higher risks. This observation is a reminder that the overall clinical picture cannot be reduced to one isolated measurement. Instead, the small distinctions in patient profiles must be acknowledged when assessing risk and planning treatments.
The mixed data on cardiovascular events underscores the need for a nuanced approach. Rather than taking an overly simplistic view of midodrine as either completely beneficial or entirely harmful, clinicians need to take a closer look at individual risk factors. The following bullet list summarizes key considerations in this area:
- Assess comorbidity profiles thoroughly before prescribing midodrine.
- Monitor for signs of both improved and worsening cardiovascular function.
- Consider whether the midodrine dose is marking a higher baseline risk of vascular instability.
- Adjust treatment protocols based on both short-term blood pressure improvements and long-term mortality risks.
This data invites us to figure a path where a balance is struck between short-term symptom control and long-term outcomes. The study clearly calls for additional, prospective research that takes into account full-scale patient data, including comprehensive monitoring of intradialytic hypotension events.
Considering the Broader Picture: Patient-Centered Care in Hemodialysis
At the heart of these discussions is a simple principle: patient-centered care is critical. Every patient on hemodialysis comes with a unique set of medical puzzles, and managing these tricky parts requires more than a one-size-fits-all approach.
For example, several patients on midodrine also receive anti-hypertensive medications. The combination of these drugs could lead to increased blood pressure variability—a factor associated with worse outcomes. In such cases, the importance of tailoring treatment to the individual becomes super important. It’s not only about titrating the dose of midodrine but also about balancing it against other medications and non-drug interventions.
Moreover, treatment decisions must consider the patient’s quality of life. Imagine dealing with a nerve-racking regimen that includes frequent changes in medications, dietary restrictions, and numerous dialysis complications. Once you start to poke around the hidden complexities of each patient’s situation, you realize that the management plan must be as unique as the patient themselves.
Healthcare providers are encouraged to work in multidisciplinary teams. Nephrologists, cardiologists, dieticians, and nursing staff working together can figure a path that optimizes outcomes. Emphasizing communication among all participants—and with patients themselves—can make a meaningful difference in treatment adherence and success.
Shaping the Future: The Need for Prospective Studies and Innovative Approaches
The study’s retrospective design inevitably limits the conclusions that can be drawn about the direct cause-and-effect relationship between midodrine and increased mortality. What is clear, though, is that there is a pressing need for prospective clinical trials. Such trials would allow us to dive in and evaluate midodrine’s direct effects in a controlled setting where confounding factors are minimized.
Future studies should aim to address several of the following points:
- Comprehensive Data Collection: Including detailed intradialytic blood pressure measurements and clinical indicators which could clarify the link between midodrine use and adverse outcomes.
- Patient Stratification: Breaking down cohorts based on the presence of diabetes, hypertension, cardiac autonomic dysfunction, and overall comorbidity burden. This step will help untangle the subtle differences that might influence outcomes.
- Comparative Studies: Comparing midodrine with alternative treatments (like dialysate cooling or adjusting ultrafiltration) can provide insight into which methods are most effective for specific patient groups.
- Long-Term Outcome Analysis: Beyond blood pressure stabilization, studies should focus on mortality, hospitalization rates, and quality of life to truly evaluate the cost-benefit profile of midodrine.
Such studies would not only clarify the effects of midodrine but also help in drafting better clinical guidelines. Given that midodrine use might be influenced by regulatory decisions and physician preferences, a standardized approach backed by high-quality evidence would be a win for patient care.
Working Through the Confusing Bits: Practical Recommendations for Clinicians
In the meantime, while further research is awaited, clinicians can follow several best practices based on the current evidence. The following bullet list summarizes a set of recommendations designed to address both the immediate and long-term challenges posed by midodrine use:
- Start Low, Go Slow: Initiate midodrine at a low dose and monitor the patient’s response closely to avoid the pitfalls of overtreatment.
- Monitor Continuously: Regularly assess blood pressure trends and cardiovascular responses during and after dialysis sessions.
- Evaluate Comorbidities: Take into account other health issues, especially diabetes and cardiovascular conditions, which might compound risks.
- Integrate Adjunct Measures: In addition to pharmacotherapy, use strategies such as fluid management adjustments and dialysate cooling.
- Review Anti-Hypertensive Use: Reassess the need for concurrent antihypertensive drugs, since a combination with midodrine might add to blood pressure fluctuations.
- Educate and Involve Patients: Engage patients in their treatment plan by discussing the potential benefits and risks of midodrine as well as alternative approaches.
By taking these measures, clinicians can better manage the tricky parts associated with hemodialysis-related hypotension and aim for improved long-term outcomes. It also underscores the importance of individualized care and continuous re-assessment of each treatment’s risk-benefit ratio.
Collaboration as the Key to Improving Clinical Outcomes
No single medical professional can hope to solve all the twists and turns associated with managing hypotension in dialysis patients alone. Effective patient care requires collaboration across specialties. When nephrologists team up with cardiologists, especially for patients who might have underlying heart conditions, the chances of making informed decisions increase dramatically.
For example, much of the debate around midodrine is rooted in its potential effects on tissue perfusion. A cardiologist’s input on how vasoconstrictors might alter cardiac output, coupled with a nephrologist’s perspective on fluid balance, can result in a more comprehensive management plan. Equally, dieticians can contribute by advising on interdialytic weight gain and nutritional modifications that help stabilize blood pressure. This interdisciplinary approach is not only practical but essential for tackling the loaded challenges that many patients face.
In addition, regular case reviews and team meetings can help identify trends and improve treatment protocols over time. As more data become available—especially from prospective studies—these collaborative efforts will help refine current practices and lead to innovative strategies that benefit patient care.
Final Thoughts: Balancing Immediate Relief with Long-Term Health
Midodrine remains a popular therapeutic option for managing intradialytic hypotension in patients undergoing hemodialysis, but its association with increased all-cause mortality certainly raises important concerns. The dose-dependent trends observed remind us that while immediate symptomatic relief is essential, it should not come at the expense of long-term patient health.
In our quest for a balanced treatment pathway, it is critical for clinicians to take a step back and consider the overall clinical scenario. This means carefully evaluating the need for midodrine, tailoring the dose with precision, and integrating non-pharmacological strategies that address the underlying causes of IDH. Another key consideration is the systematic review of comorbid conditions and mitigating the fine points of cardiovascular risk before committing to any single therapy.
Ultimately, while midodrine can be a useful tool, it should be viewed as part of a broader treatment strategy aimed at improving hemodynamic stability without compromising overall survival. As we take a closer look at the data and work through the maze of interconnected issues, the message is clear: enhance patient care by striving for holistic, interdisciplinary, and personalized treatment plans.
It is our hope that future prospective studies will provide a clearer picture of midodrine’s safety profile and further guide our clinical decisions. Until then, staying vigilant, continuously reassessing treatment protocols, and maintaining strong channels of collaboration remain our best strategies for working through the confusing bits of managing intradialytic hypotension.
In conclusion, while midodrine offers a means to elevate blood pressure during dialysis sessions, its association with poor long-term outcomes calls for cautious use. Clinicians must actively search for, and address, additional risk factors and comorbidities. With a combination of careful dosing, patient-centered strategies, and interdisciplinary collaboration, we can hope to improve both short-term stability and overall survival for patients on maintenance hemodialysis.
Originally Post From https://www.nature.com/articles/s41598-025-08029-8
Read more about this topic at
Safety of midodrine in patients with heart failure …
Midodrine and clinical outcomes in patients on …
