
Suprachoroidal Implants: A Novel Approach in Macular Edema Treatment
In recent years, the field of ophthalmology has seen exciting shifts in the management of cystoid macular edema (CME). As we continue to get into the fine points of modern treatment options, suprachoroidal corticosteroid implants have emerged as a promising alternative for patients with tricky parts in their iris–lens diaphragm. This opinion editorial will take a closer look at how these implants are changing the game, especially for patients with eyes that present tangled issues compromising traditional intravitreal approaches.
Understanding the Foundations of Suprachoroidal Implantation
Traditional methods of treating CME, which include intravitreal injections of corticosteroid slow-release implants, have greatly improved outcomes for many patients. However, when a patient has a disrupted iris–lens diaphragm—due to factors such as scleral fixated lenses, large iridotomies, or aphakia—the situation becomes full of problems, as these implant placements can lead to anterior chamber migration and subsequent damage to the corneal endothelium.
When implants accidentally shift forward, they can cause a cascade of issues that include corneal decompensation. In severe cases, patients might even require procedures like posterior lamellar keratoplasty to safeguard their vision. It’s crucial to address these complications by thinking outside the box, which is why the suprachoroidal route has garnered interest. Placing the implant between the choroid and the sclera may offer a safer, more stable alternative for such high-risk cases.
Exploring the Technical Aspects: A Practical Look at the Procedure
The suprachoroidal implantation process relies heavily on precision. Working through the surgical procedure involves a set of steps that, when performed correctly, can dramatically reduce the risk of complications associated with traditional intravitreal insertions. Here is an overview of the procedure:
- Patient Selection: Those with chronic CME and disrupted iris–lens barriers due to factors like scleral fixated lenses, large iridotomies, or aphakia are considered ideal candidates.
- Surgical Preparation: The use of a 3D heads-up system enables the surgeon to get into the nitty-gritty of ocular structures, ensuring the surgical field is clear and visible. This step helps in minimizing the risk of implant migration.
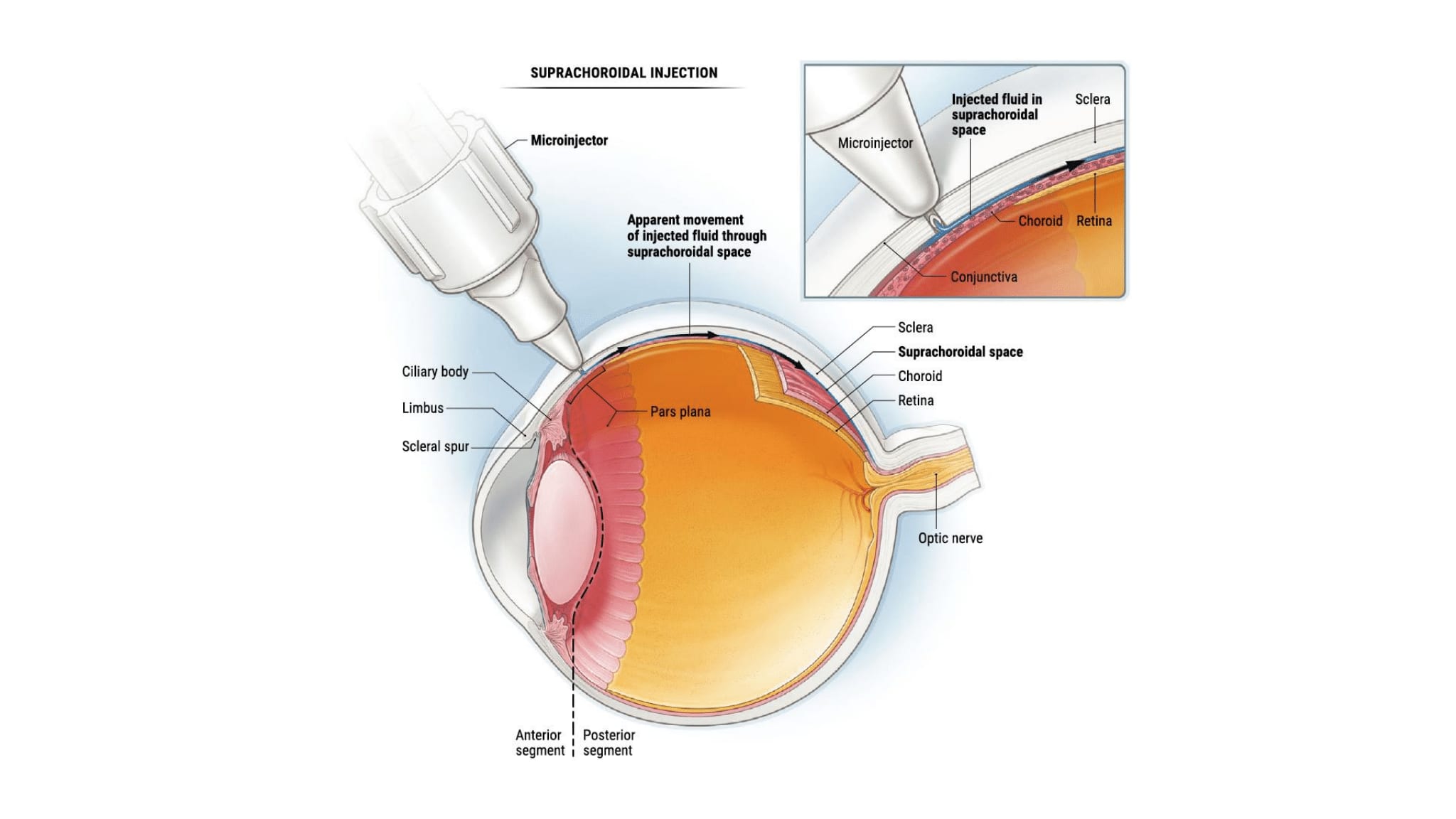
- Sclerotomy and Viscoelastic Injection: After a small, well-measured incision is made, careful separation of the suprachoroidal space is achieved by injecting dispersive viscoelastic material. This vital step helps to define the surgical plane.
- Implant Insertion: A slow-release implant (either dexamethasone or fluocinolone acetonide) is gently inserted into the suprachoroidal space, reducing the chance of structural stress on the implant.
- Wound Closure: The surgical incision is closed with a self-absorbing suture, ensuring a secure placement and helping to prevent any post-operative migration.
This step-by-step overview not only sheds light on the operational aspects but also highlights how medical professionals are starting to figure a path around potential complications posed by disrupted ocular structures.
The Benefits of a Suprachoroidal Approach in Challenging Cases
For patients with CME and associated eye abnormalities, the suprachoroidal route has several compelling advantages. Let’s dive in to unpack some of the essential and key benefits:
- Improved Stability: Placing the implant in the suprachoroidal space minimizes the risk of unwanted forward movement into the anterior chamber. This improved stability is critical in preventing damage to the corneal endothelium.
- Enhanced Safety Profile: By avoiding intravitreal migration, this method reduces the likelihood of long-lasting corneal complications, such as severe edema, which can compromise vision.
- Prolonged Drug Efficacy: The slow-release nature of these implants means that the medication is delivered consistently over time, which is beneficial in chronic conditions that require sustained treatment.
- Reduced Steroid-Related Side Effects: Data thus far indicate a lower incidence of steroid-induced glaucoma when using the suprachoroidal route, thanks to diminished exposure of the anterior tissues to high steroid concentrations.
For many patients facing overwhelming consequences from traditional methods, this approach presents an effective and safe alternative. It is a super important development in the realm of retinal disease management, particularly for those with unstable ocular anatomy.
Key Surgical Considerations: Tackling the Tricky Parts
Every innovative medical technique comes with its own set of twists and turns. Suprachoroidal implantation is no different. There are several technical challenges that surgeons must heed to ensure a successful outcome:
Optimizing Sclerotomy Size
One of the most critical factors in the procedure is choosing the correct incision size. Too small, and the implant insertion becomes nerve-racking due to the excess force needed, potentially damaging the implant. Ideally, a 2.5–3.0 mm incision is recommended. This dimension ensures a smooth insertion while keeping the implant intact.
Enhancing Visualization
Securing an accurate view of the suprachoroidal space is another bit full of problems that surgeons face. Poor visualization can result in misplacement of the implant. Utilizing high-quality illumination and magnification, often by means of a surgical microscope, helps guide the surgeon’s hand. A small viscoelastic injection further enhances the clarity of the space, enabling the surgeon to poke around with more confidence.
Ensuring Posterior Implantation
By directing the implant to a posterior position—typically 3–4 mm behind the limbus—the risk of anterior misplacement is minimized. Anterior placement can lead to choroidal detachment and other untoward consequences. This careful attention to the small distinctions in placement is one of the key reasons suprachoroidal implantation is growing in popularity among eye specialists.
Comparing Traditional Intravitreal Implants to the Suprachoroidal Method
Traditionally, intravitreal injections have been the method of choice for delivering corticosteroid implants for CME. However, these approaches carry a risk of implant migration in eyes with unstable iris–lens configurations. Let’s look at a summary table that highlights the differences between the two methods:
| Parameter | Intravitreal Implant | Suprachoroidal Implant |
|---|---|---|
| Implant Stability | Risk of anterior migration | Enhanced stability in the suprachoroidal space |
| Risk of Corneal Damage | Higher risk due to migration into the anterior chamber | Lower risk with proper posterior placement |
| Intraocular Pressure Changes | Potential for steroid-induced glaucoma | Minimal changes in intraocular pressure observed |
| Ease of Implantation | Standard injection with known challenges | Requires precise technique and visualization tools |
| Duration of Action | Long-lasting but sometimes inconsistent due to migration | Consistent drug release with sustained outcomes |
This table helps to clearly differentiate the benefits and drawbacks of each method. While traditional methods have their successes, the suprachoroidal approach offers a promising solution for those patients facing extra-tangled issues due to their unique ocular anatomies.
Assessing the Safety and Efficacy: What Do the Numbers Say?
One of the most critical measures in evaluating any new treatment is its success in both anatomical and functional outcomes. A recent case series demonstrated these points effectively. The study involved 16 patients who underwent the suprachoroidal implantation of corticosteroid slow-release devices, with follow-up data showing significant improvements in retinal thickness and visual acuity.
A quick look at the numbers:
- Central Retinal Thickness (CRT): Reduced from approximately 563 μm to 382 μm, showcasing a significant decrease in edema.
- Best Corrected Visual Acuity (BCVA): Marked improvement from 1.07 logMAR to around 0.65 logMAR.
- Intraocular Pressure (IOP): No significant rise was observed, suggesting a lower risk of steroid-induced glaucoma.
The adjusted metrics indicate that, even in eyes with unstable iris–lens diaphragms, the suprachoroidal approach can effectively reduce CME and enhance vision. This data supports the notion that this method is not only innovative but also reliable in handling the more challenging cases.
Patient-Centered Considerations: Balancing Pros and Cons
The decision to use a suprachoroidal implant over traditional intravitreal methods should always be patient-centric. For individuals with specific anatomical challenges, the benefits of the suprachoroidal approach can be particularly influential. Here are a few key considerations:
- Surgical Relief: For patients who have previously experienced complications like implant migration or corneal decompensation, the extra safety measures provided by the suprachoroidal method offer significant reassurance.
- Improved Quality of Life: With sustained visual improvement and lower side effects, patients may enjoy better daily functioning and reduced anxiety surrounding their treatment outcomes.
- Reduced Need for Repeat Procedures: Given the lower risk of implant migration, patients might not have to face repetitive surgeries, a benefit that is both financially and emotionally relieving.
When discussing this innovative approach with patients, ophthalmologists must clearly explain the potential twists and turns of the procedure, along with the specific benefits tailored to their unique ocular conditions. This open dialogue ensures that patients understand the key differences and may help alleviate overwhelming fears about undergoing a new type of intervention.
Training and Experience: Overcoming the Nerve-Racking Learning Curve
One common concern among surgeons is the nerve-racking nature of adopting new techniques. However, for those with ample experience in managing the suprachoroidal space, the learning curve may not be as steep. It is advisable for less experienced surgeons to work under supervision during the early cases. This approach allows them to:
- Gain confidence in handling the small details of the procedure
- Figure a path through the new surgical steps safely
- Benefit from mentorship while sorting out the tricky parts
This mentorship model not only enhances patient safety but also builds a solid foundation for adopting innovative techniques in clinical practice. It is all about taking that first step and gradually becoming comfortable with the method, even when the process feels intimidating or overwhelming at first.
Addressing the Challenges: The Confusing Bits of Implant Degradation and Biocompatibility
One of the ongoing questions in the field is how long the implant remains stable within the suprachoroidal space. While intravitreal implants biodegrade within approximately six months, the same rate of degradation in the suprachoroidal space is not fully established. Some experts speculate that the rate should be similar, but more research is needed to confirm these fine shades of difference.
Additionally, implants such as the fluocinolone acetonide device may leave behind a biocompatible shell after complete absorption. Although this residue is generally considered acceptable in the vitreous, its behavior in the suprachoroidal space is still under careful observation. Ongoing patient follow-up and technological advances—such as improvements in swept-source OCT imaging—help doctors track the implant’s exact positioning and degradation over time.
This monitoring is essential, as any unforeseen complications related to the implant’s breakdown or biocompatibility must be identified early. For now, early patient results have been promising, with no significant side effects observed even up to 10 months postoperatively.
Current Research and Future Directions in Suprachoroidal Implantation
The current body of research—though still limited—signals promise for the suprachoroidal approach. However, experts agree that additional prospective, randomized, double-blinded studies are necessary to solidify our understanding of both efficacy and long-term safety. Looking ahead, research focus areas include:
- Long-term Outcomes: Studies looking specifically at the durability of suprachoroidal implants and their long-term benefits will help determine the optimal patient profiles for this treatment.
- Comparative Effectiveness: Direct comparisons with traditional intravitreal methods in larger, randomized trials will be needed to tease apart the subtle differences in treatment outcomes.
- Innovation in Imaging Technology: Enhanced imaging techniques can offer more precise insights into implant positioning, degradation kinetics, and potential side effects, further refining the surgical technique.
- Patient Satisfaction and Quality of Life: Beyond anatomical improvement, future research will also need to focus on patient-reported outcomes to gauge the true impact of the new approach on day-to-day living.
As researchers dig into these challenging areas, the medical community as a whole stands to benefit from a broader range of treatment options for patients suffering from CME, particularly those with problematic ocular configurations.
Real-World Experiences: Voices from the Clinic
Every new procedure eventually adapts to the realities of everyday clinical care. Several ophthalmologists who have adopted the suprachoroidal technique report that the procedure is generally well tolerated by patients, and that the immediate post-operative period is often marked by minimal discomfort. While complications such as conjunctival hemorrhage or mild corneal erosion have been noted, they are typically minor and resolve with conservative management.
Feedback from patients also reflects a high degree of satisfaction, driven by:
- Noticeable improvements in visual clarity
- A significant reduction in the frequency of required follow-ups for issues like implant migration
- The reassurance that comes from knowing the treatment is tailored to address their specific anatomical challenges
Such real-life accounts prove invaluable when healthcare providers are trying to figure a path toward integrating innovative treatment methods. Echoing the experiences of early adopters, the suprachoroidal technique appears to complement traditional approaches, particularly in cases where the usual treatment plan might not be viable.
Addressing the Broader Impact on Healthcare Policies and Practices
Change in healthcare often requires shifts not only in clinical practice but in the related policies and funding allocations. As suprachoroidal corticosteroid implants gain momentum, several broader issues come into play:
- Insurance and Reimbursement: With newer techniques often facing challenges in securing broad insurance coverage, it is critical for healthcare institutions to work closely with payers to recognize the long-term cost benefits of reduced complications and fewer repeat interventions.
- Training Programs: Incorporating suprachoroidal implantation protocols in residency and fellowship training courses will help the next generation of eye care specialists get around the confusing bits of newer surgical techniques.
- Interdisciplinary Collaboration: As advancements in ophthalmology influence other fields such as pharmacology and imaging technology, a collaborative approach will be necessary to develop standardized procedures that can be widely adopted.
These broader discussions highlight the importance of nurturing innovation in healthcare while ensuring that new treatments meet rigorous standards of safety and efficiency. By striking a balance, medical professionals and policymakers can collaboratively steer through the evolving landscape of ocular treatment methodologies.
Looking Ahead: A Future of Tailored Treatments and Enhanced Outcomes
Suprachoroidal implantation represents more than just another tool in the treatment arsenal; it signals the dawn of a more tailored approach for managing complex retinal conditions. As we continue to poke around the potential of these innovative therapies, several future directions become clear:
- Customized Patient Care: By honing in on individual anatomical challenges, surgeons can offer treatments that are specifically designed to mitigate the complications of conventional methods. This customization is set to elevate patient outcomes to new heights.
- Integration of Technology: The role of advanced imaging, such as swept-source OCT, highlights how technological integration is essential in monitoring treatment progress. These imaging breakthroughs allow for the precise tracking of implant position and integrity over time.
- Enhanced Drug Delivery Systems: Future innovations in the design of slow-release implants could further optimize drug kinetics, ensuring that patients receive the optimal dosage over an even longer period.
- Multicenter Trials: To move beyond initial case series, coordinated efforts involving multiple centers and larger patient cohorts are needed. Such studies will help fine-tune the surgical protocol and confirm the benefits observed in early clinical experiences.
Ultimately, the push for more robust research underscores the dynamic nature of modern medicine. As new treatment paradigms are explored, the hope is that every patient—no matter how complicated their ocular structure—will have access to safe, effective, and personalized care.
Conclusion: Embracing Change in the Face of Ocular Challenges
The journey toward optimizing the treatment of cystoid macular edema is filled with twists and turns, particularly when dealing with eyes that present extra-tangled issues such as a disrupted iris–lens diaphragm. The advent of suprachoroidal corticosteroid implants marks a significant leap forward, offering a safe, effective, and innovative alternative for a patient subgroup that previously faced overwhelming risks with traditional therapies.
Although every new method comes with a few nerve-racking challenges—from selecting the right sclerotomy size to ensuring proper implant placement—the benefits of improved stability, enhanced safety, and prolonged drug efficacy cannot be overstated. Early clinical data and real-world experiences strongly support the use of this approach in complex cases, while future multicenter studies and technological advancements promise to refine and expand its application.
For medical professionals, the key lies in remaining open to integrating novel techniques while keeping patient well-being at the forefront. As we continue to get into the subtle parts of CME management, suprachoroidal implantation stands out as a critical, must-have option in the fight against vision-threatening complications. By embracing these advancements, the ophthalmology community can ensure a brighter, clearer future for patients, no matter how tricky their ocular challenges may be.
Originally Post From https://www.nature.com/articles/s41598-025-05611-y
Read more about this topic at
Suprachoroidal Injection: A Novel Approach for Targeted …
Suprachoroidal Injection: A Novel Approach for Targeted …